Knee replacement: Are misalignments always completely corrected?
Why a completely straight leg is not necessarily required after an artificial knee joint (knee replacement)
Knee replacement surgery has advanced enormously in recent decades. Patients with severe osteoarthritis or other degenerative diseases of the knee joint benefit from modern knee prostheses (total knee arthroplasty), which alleviate pain and improve mobility. A key aspect of knee replacement surgery is the correction of knee joint misalignment.
Traditionally, a neutral mechanical axis was the goal to ensure even loading of the knee prosthesis. However, newer approaches are increasingly questioning this practice and favoring concepts such as kinematic alignment, in which existing axial deviations are left within a certain range. This article provides a comprehensive overview of various resection techniques, the correction of malalignments, and current developments in knee arthroplasty.
Anatomy and biomechanics of the knee joint
The knee joint is the largest joint in the human body, connecting the thigh bone (femur) to the shin bone (tibia). It is a complex hinge joint that allows for flexion, extension, and slight rotational movements. The stability of the knee joint is ensured by various structures such as ligaments, menisci, and muscles.
The natural axis of the leg often exhibits a slight O-shape (varus) or X-shape (valgus). These natural deviations can vary from person to person and affect joint stress as well as soft tissue tension. If this is not optimally addressed, it can lead to long-term problems, which is why alternative alignment strategies are becoming increasingly important.
Knee joint misalignment: causes and effects
Knee joint misalignments can be congenital or develop over the course of a lifetime. Common causes include:
- Degenerative diseases : Osteoarthritis leads to cartilage degeneration and can alter joint geometry.
- Trauma : If left untreated or inadequately cared for, injuries can lead to deformities.
- Inflammatory diseases : Rheumatoid arthritis and other systemic diseases can cause lasting damage to the joint structure.
These misalignments significantly affect joint mechanics, lead to uneven stress, and can accelerate wear and tear. A balanced approach to correction is therefore essential.
How does a knee prosthesis work?
A knee prosthesis is an artificial joint replacement used to restore the function of a knee joint damaged by osteoarthritis, injury, or other diseases. Modern knee prostheses consist of several components that are precisely coordinated to allow for natural mobility and stability.
1. Construction of a knee prosthesis
A knee prosthesis typically consists of three main components:
- Femoral component (thigh part): This metal component replaces the damaged joint surfaces of the thigh bone (femur) and glides over the polyethylene surface of the tibial component.
- Tibial component (shinbone portion): This metal platform is placed on the upper end of the shinbone and serves as a stable base for the artificial polyethylene gliding core.
- Patellar component (kneecap part): Optionally, the kneecap can also be replaced by a polyethylene component to ensure optimal gliding ability.
Additionally, there are different degrees of coupling , which vary depending on how much the prosthesis has to replace the stability of the natural knee ligaments.
2. How a knee prosthesis works
The knee prosthesis works by replicating the mobility of the natural knee joint. Modern total knee replacements (TKRs) are designed to:
- low -friction gliding movement between the artificial joint surfaces.
- To preserve or reconstruct the physiological axis
- the natural band tension into account, especially during kinematic alignment.
- High stability while standing and fluid mobility while walking are guaranteed.
3. Range of motion and stability after knee replacement
Following successful implantation, a knee prosthesis can allow flexion of 120° or more , depending on the patient and surgical method. Modern implants are designed for a lifespan of over 20–30 years and are made of wear-resistant materials such as highly cross-linked polyethylene and cobalt-chromium alloys .
4. Different orientation methods of the knee prosthesis
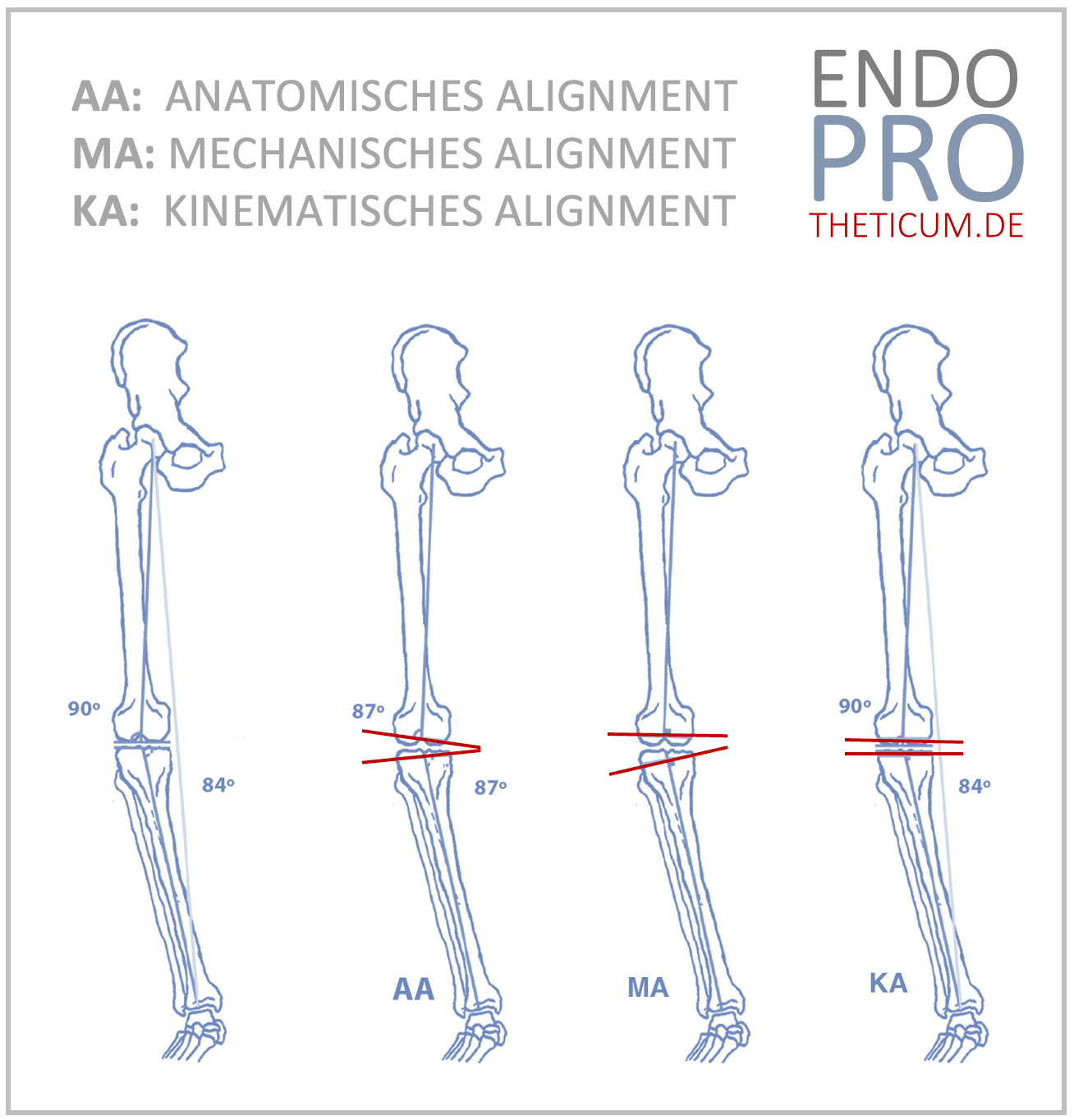
Depending on anatomical conditions and individual misalignment, knee prostheses are now aligned according to different principles:
- Measured Resection (Mechanical Alignment):
→ Here, the knee joint is aligned so that the leg has a straight axis , regardless of its original position. - Kinematic alignment:
→ Natural ligament tension is largely maintained by allowing slight bowlegs or knock-knees to persist. This often leads to a more natural feeling of movement.
5. What does a knee replacement feel like?
Patients often report a significant reduction in pain and an improved quality of life after total knee replacement. In the first few months, the implant may feel unfamiliar, but with targeted physiotherapy, a near-normal range of motion can often be achieved.
Measured Resection: The traditional technique for knee replacement
The measured resection technique is one of the oldest methods for knee replacement surgery. In this technique, the knee is aligned to achieve a mechanically neutral axis, regardless of the patient's original anatomy.
Procedure
- Bone sections : The bones are resected according to predefined angles and dimensions.
- Alignment : Special instruments ensure that the bone cuts are performed in an optimal axis.
- Soft tissue balancing : After the bone cuts, the soft tissues, especially the ligaments, are adjusted to achieve even tension.
Advantages
- Standardized, proven technology with good long-term results.
- Highly reproducible results.
- Even loading of the prosthetic components.
Disadvantages
- Potentially increased soft tissue stress due to forced adaptation to a standardized axis.
- Can lead to unphysiological joint stress.
- Not every patient benefits from a complete axis correction.
Kinematic Alignment: An individualized approach to knee replacement
Kinematic alignment involves adapting the knee prosthesis design to closely replicate the patient's natural anatomy. This technique allows for maintaining a slight varus or valgus position to preserve natural ligament tension and soft tissue balance.
Procedure
- Patient-specific planning : Highly developed imaging techniques help to determine the natural axis.
- Minimally invasive soft tissue adjustment : The soft tissues are not unnecessarily stretched or tightened in order to ensure even stress distribution.
- Individual bone cuts : The resection is performed along the natural knee axis.
Advantages
- Reduces tension on ligaments and muscles.
- This can lead to a shorter rehabilitation time.
- Allows for more natural joint movement.
Disadvantages
- Requires more precise preoperative planning.
- May not be suitable for certain patients.
- The long-term results are not yet as comprehensively documented as with the traditional method.
The trend towards partial correction of malpositions in knee endoprosthetics
In recent years, there has been a growing understanding that complete correction is not always the best solution. Particularly in kinematic alignment, a moderate misalignment is often maintained to avoid impairing natural joint dynamics.
- Varus correction : A severe bowleg becomes a mild bowleg.
- Valgus correction : A severe X-leg becomes a mild X-leg.
These moderate corrections can help prevent the soft tissues from becoming unnaturally stretched and maintain mobility.
Future prospects in knee arthroplasty
The future of knee arthroplasty will be strongly influenced by personalized implant designs, robot-assisted surgery, and advanced biomechanical insights. Individualized solutions such as kinematic alignment will be further optimized and increasingly integrated into routine clinical practice.
Conclusion
Complete correction of malalignment associated with knee replacement (total knee arthroplasty) is not always the best solution. Modern techniques such as kinematic alignment allow for a more individualized approach to artificial knee joints, which offers advantages for many patients. The choice of the right technique should be made on an individual basis to achieve the best possible long-term results.
MAKE AN APPOINTMENT?
You are welcome to make an appointment either by phone or online .


ENDOPROTHETICUM - The whole world of endoprosthetics