Small prosthesis: less is often more!
The modern part of the knee in the focus: the sled prosthesis

The sled prosthesis - also referred to as a unicondylary knee joint replacement or partial joint replacement - is a modern and tissue -shaped solution for patients with isolated osteoarthritis in the knee joint. While many patients initially think of a complete joint replacement, the sled prosthesis offers a minimally invasive and functionally convincing alternative. This detailed article shows you why the sled prosthesis often applies: less is more. You will also learn how modern surgical techniques, new implant materials and precise diagnostics lead to better results and faster rehabilitation.
The focus of the knee - if every movement hurts
The knee joint is one of the most complex and most stressed joints in the human body. Millions of people suffer from osteoarthritis - a degenerative joint disease that leads to pain, restrictions on movement and ultimately a significant loss of quality of life. While the complete joint replacement is often necessary when the arthrosis is advanced, there is a significantly gentler alternative for certain patient groups: the sled prosthesis , also known as unicondylary knee prosthesis or partial joint replacement .
What is a sled prosthesis?
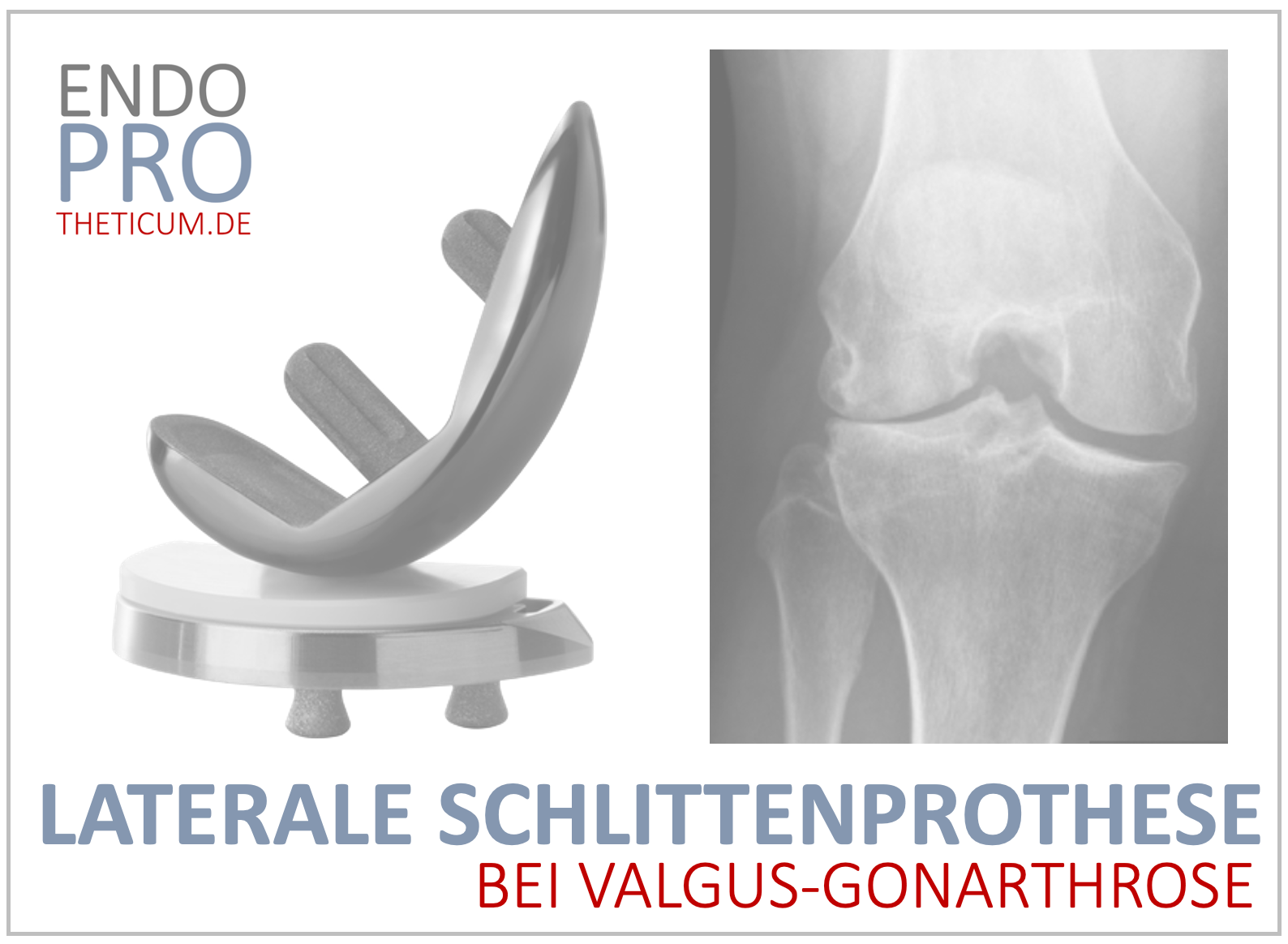
The sled prosthesis is a form of the artificial knee joint, in which only part of the joint is replaced - usually the inner or outer joint side (media or lateral). In contrast to a total endoprosthesis (knee-tep), in which all the articular surfaces are replaced, the healthy structures such as the cross ligaments, side ligaments and the unknown joint section remain during the sled prosthesis.
This procedure is particularly suitable for patients who only suffer from one -sided osteoarthritis and whose remaining knee joint is intact. The lower bone loss is also advantageous, which simplifies later revision operations.
Building the sled prosthesis
- Metal components : The thigh and lower leg shares are usually made of high-quality titanium or cobalt chrome.
- Plastic inlay (polyethylene) : serves as a sliding area between the two metal components.
- Fixing : Usually cemented, and in individual cases also possible.
Indications for a sled prosthesis
Not every patient with knee arthrosis is automatically a candidate for a sled prosthesis. The ideal requirements are:
- Isolated media or lateral gonarthrosis
- Maintenance of the front and rear cross ligaments
- Intact lateral or media compartments
- No significant axis misalignment or instability
- Good general condition and motivation for rehabilitation
Precise imaging- ideally in the form of an MRI or X-ray diagnostics with stress recordings- is essential to assess the scope of cartilage damage and the integrity of the remaining joint structures.
When is a sled prosthesis suitable?
A slide prosthesis is particularly suitable for patients with:
- Isolated osteoarthritis : If only part of the knee joint is affected.
- Intacted band apparatus : The front cruciate ligament in particular should be functional.
- Good bone substance : A sufficient bone density is necessary for the anchoring of the prosthesis.
- Active lifestyle : patients who want to remain active benefit from the mobility of the sled prosthesis.
Advantages of the sled prosthesis
1.
The sled prosthesis leaves large parts of the native knee joint intact, which enables a more natural feeling of movement and physiological joint kinematics.
2. Lower intervention
The operational access is smaller, fewer soft tissues are violated and blood loss is lower.
3. Faster rehabilitation
Many patients can quickly burden the operated leg again and return faster in everyday life and work.
4. better revision opportunities
Since only part of the joint is replaced, more bones are preserved. If there are further signs of wear in the course, conversion into a total endoprosthesis is easier.
Operative technology of the sled prosthesis - precision is crucial
The implantation is usually minimally invasive and using modern aids such as computer navigation or robot-based technology. The correct axle position and alignment of the components is crucial in order to achieve ideal biomechanics.
The affected compartment - medially or laterally - is smoothed, prepared and equipped with a tailor -made prosthesis. Usually cemented is fixed, but there are also cement -free designs.
Material choice: modern implants for maximum durability
Current sled prostheses consist of highly networked polyethylene inlays in combination with titanium or cobalt chrome components. The sliding surfaces are extremely abrasion -resistant, which significantly extends the lifespan of the prostheses. Long -term studies show a service life of over 15 years with high patient satisfaction.
Postoperative care and rehab with sled prosthesis
Mobilization with forearm support is already possible on the day of the operation. Depending on the operational technology, the full load is usually allowed immediately or a few days. Early physiotherapeutic care aims to quickly restore mobility, muscle strength and coordination.
Rehabilitation usually lasts 3-4 weeks and can be inpatient or outpatient. The goal is to return to everyday life, work and leisure activities as early as possible.
Comparison between sled prosthesis and total endoprosthesis (TEP)
A central point in the decision for or against a sled prosthesis is the comparison with the total endoprosthesis (TEP) of the knee. Both procedures are used in osteoarthritis, but differ fundamentally in the indication, surgical effort, recovery time and long -term result.
Anatomical differences
The total endoprosthesis replaces the entire joint surface of the knee joint- both on the thigh and the shin side. The sled prosthesis, on the other hand, is limited to one of the three joint shares (usually the media share), whereby the remaining joint structures - especially cross -ligaments, lateral joint content and kneecap - are preserved.
Surgical extent
The operation for the implantation of a sled prosthesis is much smaller because only part of the joint is replaced. It is often minimally invasive, with smaller cuts, less soft tissue damage and significantly reduced risk of bleeding. The procedure is therefore often shorter, less risky and better tolerated for the patient.
Functionality and feeling of movement
Because the natural ligaments and bone structures are preserved in the sled prosthesis, many patients feel their knees after surgery as "natural". The proprioceptive feedback is better, the gait image more physiological. A total endoprosthesis, on the other hand, offers more comprehensive care with advanced osteoarthritis, but is accompanied by an artificial feeling of movement.
Rehabilitation duration
The rehabilitation after a sled prosthesis is usually faster and easier. Patients need longer rehabilitation stays and previously reach their full resilience. The climbing stairs and executing sporting activities is usually easier and faster.
Complication rate
The complication rate - especially infections and thrombosis - is statistically lower in the sled prosthesis. Revision operations are also easier to carry out because less bones are removed. In contrast, an exchange operation with a TEP is technically complex.
Long -term indications
The TEP is indicated in cases in which there is already a tricoming type throat throat or there are band instabilities. In the case of localized osteoarthritis, the sled prosthesis, on the other hand, is the procedure of choice - not least because of the potential way to switch to a TEP later, if necessary.
When is a total endoprosthesis of the better choice?
A sled prosthesis is not always sufficient. With advanced osteoarthritis in several compartments, instabilities or band injuries, a complete knee-TEP is more sensible. A total endoprosthesis is also the better option in the case of inflammatory rheumatic underlying diseases or complex malpositions.
Sports and activity according to sledding prosthesis
Many patients can actively participate in life again after the operation. Particularly accurate sports such as hiking, swimming, cycling or Nordic walking are easily possible. Golf or cross -country skiing can also be exercised - after individual consultation. High dynamic or joint -stressing sports such as jogging or tennis should be considered with caution.
Risks and complications of a sled prosthesis - what you should know
Although it is a comparatively gentle procedure, the sled prosthesis is also a surgical intervention with certain risks:
- Loosening of the prosthesis (rare, in the event of overload)
- Progression of osteoarthritis in other compartments
- Pain in the event of malpositioning
- Infections (very rare in aseptic conditions)
Long -term results and durability of the sled prosthesis
Current studies show that modern sled prostheses have a survival rate of over 90 % after 10–15 years . The right patient selection and precise surgical technology are crucial.
Contrary to earlier assumptions, modern sled prostheses show very good long -term results today. Technological progress, improved materials and more precise surgical techniques contribute significantly to the extended durability.
Shelf life in years
Modern sled prostheses reach a service life of 15 years and more. Studies show that over 90 % of the implanted sub -prostheses are still fully functional even after 10 years. With the correct indication and precise implantation, survival rates of over 95 % after ten years are not uncommon.
Influence factors on durability
- Indication position : A precise selection of patients is crucial. Small prostheses are particularly suitable for isolated media gonarthrosis.
- Surgical experience : High number of cases and expertise by the surgeon are important quality factors.
- Body weight and level of activity : Patients with a high BMI or extreme stress on the knee joint statistically have a slightly higher revision rate.
- Implant design : Modern sled prostheses are modular, anatomically shaped and equipped with highly abrasion -proof sliding pairings, which increases the lifespan.
Revision opportunities
A great advantage of the sled prosthesis is that in the event of a failure, complex interchanging operation is not necessary. Most of the time, the sled prosthesis can be transferred to a standard ontal endoprosthesis without additional special implants being necessary.
Patient satisfaction
Patients who have received a sled prosthesis often report high satisfaction, quick return to everyday activities and sporting stress. Especially in younger patients, the subjective feeling of movement is usually better than after a total endoprosthesis.
Conclusion: The sled prosthesis as a modern solution for selected patients
The partial joint replacement with a sled prosthesis represents a minimally invasive and everyday solution for many patients with one-sided knee arthrosis. Thanks to modern surgery, precise diagnosis and high-quality materials, the natural joint feeling can often be preserved or restored. A prerequisite for success are a precise patient selection and close -meshed aftercare.
FAQs on the sled prosthesis:
What is the difference between a sled prosthesis and a knee-tep? With the sled prosthesis, only part of the knee joint is replaced, in the knee-tep the entire joint.
How long does a sled prosthesis last? The durability is on average 15–20 years - depending on the load and implant type.
When can I do sports again after the operation? Gentle sports such as cycling or swimming are often possible again after a few weeks.
Can I go hiking with a sled prosthesis? Yes, hiking is one of the recommended activities after the operation.
How big is the scar? A minimally invasive cut of approx. 8–10 cm is usually sufficient.
Are there risks? As with any operation, there are risks such as infections, thrombosis or loosening of the prosthesis - but these are rare.
MAKE AN APPOINTMENT?
You are welcome to make an appointment either by phone or online .


ENDOPROTHETICUM - The whole world of endoprosthetics